
Differentiating between Bell’s palsy vs Stroke
The two most common causes of acute facial paralysis are Bell’s palsy and stroke; differentiating between these two diagnoses can often be challenging. Because acute stroke is an extraordinarily time-sensitive and potentially life-threatening condition, the correct diagnosis must be determined to hasten treatment. To achieve that end, a distinction between stroke and Bell’s palsy first must be made. Let us further explore this topic.
BELL’S PALSY
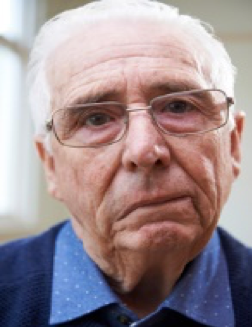
Bell’s palsy is a neurologic condition that causes temporary unilateral paralysis of the face muscles, causing them to droop and weaken.
The condition is self-limiting and brought about by inflammation or trauma to the seventh cranial nerve (facial nerve) above the stylomastoid foramen. Reactivation of Herpes Simplex Virus 1 is believed to be the infectious cause of Bell’s palsy.
Symptoms include unilateral drooping of the mouth, deviated smile, weakness in grimacing, and flattened nasolabial fold.
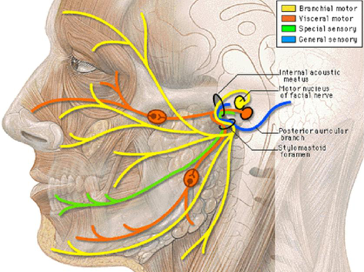
Pathway of Facial nerve and it`s innervation
STROKE
Stroke refers to the sudden onset of focal neurological deficit due to occlusion of blood supply or hemorrhage in the brain, causing signs and symptoms lasting more significant than 24 hours.
Within minutes, ischemia leads to brain cell death, making it a medical emergency for which prompt treatment is vital, with time being of the essence. Invasive treatment regimens are required.
Furthermore, stroke is one of the leading causes of death in the United States, with more than 799,000 people in the United States experiencing stroke per anum.
Stroke can be of two types: ischemic or hemorrhagic. Knowing the type of stroke is essential for its treatment.
Presentation of Bell’s palsy and Stroke
Presentation of Bell’s palsy and Stroke
| Bell’s palsy | Stroke | |
| Age group | 20-50years | >60years |
| Duration | Hours to days | Seconds to minutes |
| Upper face | Involved | May or may not be affected |
| Lower face | Always involved | Always involved |
| Ability to furrow brow | No | Yes |
| Ability to close eye on affected side | Possible | Difficulty in performing the action |
| Paralysis of other limbs | No | Yes |
| Pupils | Normal | Unequal |
| Arm drift | No | Yes |
| Other associated features | – | Ataxia, vertigo, double vision, difficulty in swallowing. |
Bell`s palsy

Upper and lower face both affected,
failure to wrinkle on affected side, deviated smile
Stroke

Drooping of lower half of face, able to wrinkle forehead on both sides
In order to form a diagnosis, it is essential to:
- Take history:
Inquire about when they initially notice the abnormalities and how fast they developed. The onset of ischemic stroke is acute and reaches maximum severity within hours. Often, witnesses may provide this vital information. It is essential to know when they were last seen normal.
- Perform a neurological examination: This will provide knowledge regarding whether the condition is peripheral or central.
If central, then most likely diagnosis would lead to stroke. At the same time, peripheral appearance would suggest Bell’s palsy, but more investigations to be made to reach a definite diagnosis.
Mouth: Facial muscle weakness can obscure the nasolabial fold. A smile would deviate. Weakness of muscles of mouth is present in both palsies.
Eyes: Initially, an inspection of the eyes is done at rest position. A subtle sign of eye closure weakness is observed. Asymmetry in the closure of eyelids is a sign of Bell’s palsy.
Forehead: Forehead lifts symmetrically in stroke. Whereas, in Bell’s palsy, the patient will not be able to wrinkle their forehead on the affected side. Asymmetrical wrinkling of the forehead is a prominent sign of peripheral Bell’s palsy.
3. Other signs or symptoms:
Weakness in the arm or leg: Ask the patient if they could lift their arm or leg to assess the weakness of muscles.
Slurred speech (dysarthria)
Double vision (diplopia): Exclude the abnormalities in extraocular muscles by asking the patient to turn the eyeballs in different directions.
Dysphagia: Trouble in swallowing.
Incoordination (ataxia): Check the coordination of limbs by asking the patient to walk.
Vertigo: Sensation of nausea or room spinning.
If the patient shows any of these signs, it is most likely a stroke as the territory involved other nerves.
Tests
☆Bell’s palsy
- Electromyography
- CT
☆Stroke
- Blood test to look at cholesterol levels
- CT or MRI
- Electroencephalogram
Treatment
Bell’s palsy
Its treatment vastly differs from that of stroke. Doctors recommend physical therapy and administration of medications (e.g., steroids, acyclovir, analgesics). The main goal in the management of Bell’s palsy is hastening the recovery and preventing corneal complications.
Approximately 70 percent of cases recover spontaneously. However, combined therapy with antiviral agents (Acyclovir) and corticosteroids (Prednisone) is recommended to reduce recovery time and increase the likelihood of healing.
Stroke
Treatment depends on the type of stroke and is much more complex. For ischemic stroke, the target is to restore the blood flow to the brain, while in hemorrhagic stroke, the goal is to achieve hemostasis and reduce the pressure being exerted on the brain.
To conclude, while assessing the acute facial weakness in a patient, examining the muscles of the face is crucial; divide it into two parts; upper and lower face, and look out for associated signs and symptoms. If muscle paralysis is limited to the lower face, the stroke would be the most probable diagnosis. If it involves the whole of the face, any associated signs and symptoms are to be sought out. Generally, Bell’s palsy occurs in the younger age group, symptoms appear slowly, and it happens in isolation without any other significant objective findings on examination.
